It’s best to respond early and aggressively to COVID-19
Click here for previous posts about COVID-19 >
Introduction
A passage from a previous post, regarding a one-page March 12, 2020 PDF overview entitled “COVID-19 Recommendations for Policy Makers,” by Chen Shen and Yaneer Bar-Yam, of the New England Complex Systems Institute, reads:
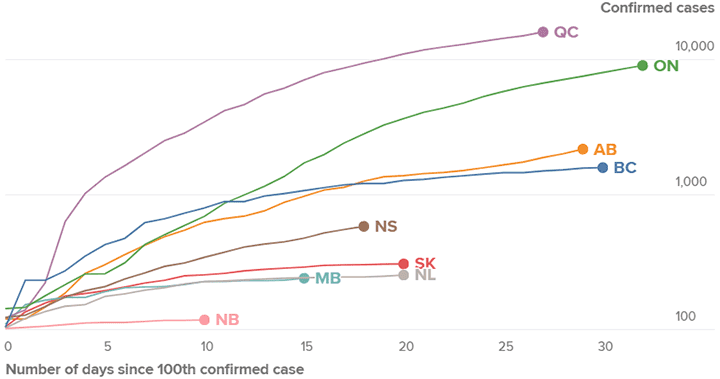
Source: April 17, 2020 Global News article entitled: “Canada is flattening the coronavirus curve. That’s ‘good news,’ expert explains.”
People are connected by an invisible transmission network whose links are the physical contacts between individuals, the breathing of common air that can contain particles that are coughed, sneezed or even just breathed out and in, as well as between individuals and physical objects that can carry viral particles deposited on them and subsequently touched by others. This transmission network is operating all the time as we engage in normal activities. It includes both workplace/professional and personal contacts with family, friends and community members. How the network is connected among individuals determines the risk that an individual will contract the disease and transmit it to others.
With regard to such a transmission network, we can see differences in responses to the pandemic.
The current post is devoted to two recent news articles, which highlight such differences. In a concluding comment, I refer to a third article as well, regarding practical matters related to COVID-19 testing.
March 13, 2020 CBC article features comments by Canadian infectious disease physician
A March 13, 2020 CBC Quirks of & Quarks article is entitled: “COVID-19: Why reacting early and aggressively is the key to avoiding crisis. We have to be proactive, rather than reactive.”
In the article, Dr. David Fisman, an infectious disease physician, shares comments regarding extensive cancellations of events in response to the pandemic:
They’re highly appropriate. We have to be proactive, rather than reactive. I’m delighted that Ontario has decided to have an extended, a three week March break to allow kids to come back from the US a good 14 days extra after they come back, to stay at home in case they have any symptoms of COVID after returning from Florida. And I think it’s exactly the right thing to do.
I think we need to do it for the sake of vulnerable folks in our society and I’m delighted to see us do it proactively rather than reactively in a time of crisis.
The infectious disease physician is asked a question about the contrast between the flu and COVID-19. He responds:
Yeah, the case fatality of this thing is probably about 20 times that of influenza. Any clinician will tell you that in a bad influenza year our hospitals are filled to the bursting. There’s a logjam, our ICUs are full. Our emergency rooms are full. People wind up basically boarding in the emergency rooms because all the beds in the hospital are full. That’s a bad flu year. This is 20 times worse.
So the idea is for this not to be bad. And that’s why we have to intervene so strongly.
We’re fundamentally a discipline that’s about prevention and having our actions result in non-occurrence of events. And I’m entirely comfortable with folks criticizing this and saying, look you cancelled our concerts, you cancelled the NHL season, you terrible person, you made restaurants empty out for a month and then nothing happened. That’s the point. By doing that we make nothing happen for a little while until this starts to heat up again.
If we allow this to get bad, it gets bad fast, and it gets horrible fast. And that’s why we have to be proactive.
He’s asked a question about how different countries have been responding to the crisis. He comments:
So, Italy is having a terrible time. There’s not enough kind of ICU beds and machinery to save the lives of people who go into respiratory failure. So people are now dying in Italy without care, because the hospitals are full to the bursting.
By contrast I think at this point, we can look at Singapore, we can look at Hong Kong, at places that have intervened early and aggressively before things became quite as dire, and seemed to have quashed local transmission quite quickly using fairly dramatic social distancing measures. But that’s allowed them to kind of move on and get back to business.
That’s why I think the decisions that are being made in Canada this week about proactively enacting social distancing measures are so important. We’re following the example of the countries that have done well.
In a discussion about what’s happening in the United States, Dr. David Fisman notes:
What I really worry about in the United States is you have tremendous variability between states in terms of the strength of public health institutions. We have a situation in Nevada for example where last week there were three Nevada linked cases reported in total. Two of them were in Las Vegas and the third one was in a Canadian who had just returned from Las Vegas. That means there is a big epidemic there because most people aren’t on a given day getting on an airplane. So if you’re exporting cases it means prevalence is high.
So I worry about those quiet places in the U.S. I worry about Florida where apparently testing capacity is very limited. And I think you have a large concentration of individuals in the age groups that get very, very sick from this virus. So I think there are a lot of blind spots in the United States. It’s a very big, very heterogeneous country and it lacks effective public health leadership right now. It’s not just a problem for the Americans, it’s a problem for us too because we’ll import those cases.
March 12, 2020 Reuters article distinguishes between responses in Italy and South Korea
A March 12, 2020 Reuters article is entitled: “Special Report: Italy and South Korea virus outbreaks reveal disparity in deaths and tactics.”
This along with the other two articles highlighted at the current post is among the most thoughtful and well-reasoned overviews that I have read in recent days.
Below is an excerpt; it’s my hope that interested site visitors will read all three articles closely as each highlights the benefits of an early and aggressive approach – in particular with regard to tracking – to the COVID-19 epidemic.
The Reuters excerpt that I’ve chosen reads:
It’s impractical to test every potential patient, but unless the authorities can find a way to see how widespread infection is, their best answer is lockdown.
Italy started out testing widely, then narrowed the focus so that now, the authorities don’t have to process hundreds of thousands of tests. But there’s a trade-off: They can’t see what’s coming and are trying to curb the movements of the country’s entire population of 60 million people to contain the disease. Even Pope Francis, who has a cold and delivered his Sunday blessing over the internet from inside the Vatican, said he felt “caged in the library.”
Thousands of miles away in South Korea, authorities have a different response to a similar-sized outbreak. They are testing hundreds of thousands of people for infections and tracking potential carriers like detectives, using cell phone and satellite technology.
Both countries saw their first cases of the disease called COVID-19 in late January. South Korea has since reported 67 deaths out of nearly 8,000 confirmed cases, after testing more than 222,000 people. In contrast, Italy has had 1,016 deaths and identified more than 15,000 cases after carrying out more than 73,000 tests on an unspecified number of people.
Epidemiologists say it is not possible to compare the numbers directly. But some say the dramatically different outcomes point to an important insight: Aggressive and sustained testing is a powerful tool for fighting the virus.
March 12, 2020 Globe and Mail article notes some front-line physicians say they’re having trouble getting patients tested
By way of conclusion, I refer to a March 12, 2020 Globe and Mail article entitled: “Doctors say coronavirus test criteria are inconsistent, could lead to dangerous gaps.”
An excerpt reads:
Despite assurances from public health officials that coronavirus tests are widely available, some front-line physicians say they’re having trouble getting patients tested, creating potentially dangerous gaps that could leave Canada vulnerable to outbreaks.
A key problem is lack of consistent communication about who qualifies for testing. For weeks, federal, provincial and local public health officials have been relying on a narrow list of countries experiencing COVID-19 outbreaks, such as China, Iran and, more recently, Italy, to help determine which individuals could be tested. The list has faced intense criticism from numerous experts who point out it doesn’t include places like Germany, France or the U.S., even though those countries are experiencing outbreaks of the coronavirus.
Florida
A March 16, 2020 Reuters article is entitled: “In Florida retirement hub, more worry about stock market collapse than getting sick from coronavirus.”
Testing and retesting in Hong Kong: April 17, 2020 Guardian article
An April 17, 2020 Guardian article is entitled: “Test and trace: lessons from Hong Kong on avoiding a coronavirus lockdown: Semi-autonomous city followed WHO advice and moved swiftly to stem contagion without rigid curbs on movement.”
An excerpt reads:
Governments in Europe and the US can learn from Hong Kong, which has kept infections and deaths from Covid-19 low without resorting to the socially and economically damaging lockdown that the UK and other countries have imposed, scientists say.
Hong Kong, with a population of nearly 7.5 million, had had just 715 confirmed cases of Covid-19 infection, including 94 asymptomatic infections, and four deaths as of March 31, according to a new study published on Friday in the Lancet.
Early in the pandemic, it was thought to be at significant risk because of travellers arriving from mainland China, but since early February the outbreak has appeared to be under control.
Leave a Reply
Want to join the discussion?Feel free to contribute!